New Hire Packet Payroll/FEA
|
|
|
- Juniper O’Neal’
- 6 years ago
- Views:
Transcription
1 New Hire Packet Payroll/FEA Submit completed forms to PICS Human Resources via , mail, or fax: Mail: 1605 Eustis St, St Paul, MN Fax: Once employment requirements are completed, PICS Human Resources will or mail Date of Hire notice to Representative and Worker. Please note that any hours worked prior to this date cannot be paid. PICS Worker Participant Representative Participant Employer Processes Payroll Provides Direct Support Receives Services Supervisor Business Holder Worker Name: Participant Name: Representative Name: Program Type: CDCS CSG Completed Completed Completed Forms for Worker Individual Support Worker Enrollment Application Provider Agreement Background Study Authorization (Optional for CSG. Must include copy of photo ID) Personnel File Notification W-4 Form Payment Options Form (Must include bank document for direct deposit) Forms for Worker and Representative I-9 Form FEIN Questionnaire Required for Representative s Records Employment Application Job Description Employment Agreement Training as Identified by Representative hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
2
3 Minnesota Health Care Programs (MHCP) Individual Support Worker Enrollment Application (CDCS and CSG) *DHS-4469A-ENG* DHS-4469A-ENG 6-15 Complete all fields to enroll an individual support worker. Complete this form online, print and then fax to MHCP. Incomplete forms will be returned. New hire (requires new background study) Rehire (requires new background study) PREVIOUS EMPLOYMENT END DATE: Individual Support Worker Information PROVIDER TYPE 38 INDIVIDUAL (COS 021 & 105) LEGAL NAME (FIRST) FULL MIDDLE LAST SOCIAL SECURITY NUMBER ADDRESS (RESIDENTIAL ADDRESS ONLY DO NOT ENTER A PO BOX) PHONE NUMBER NPI/UMPI (IF REQUESTING REINSTATEMENT) CITY STATE ZIP CODE COUNTY OF RESIDENCE DATE OF BIRTH If individual has been working in a different support position or was enrolled for MCO claims only, has the individual been continuously employed by your agency? Yes No BGS NUMBER/REQUEST ID (required only for CDCS) PROGRAM TYPE CSG CDCS (you must submit and have the individual pass a background check) Individual Support Worker Provider Statement I have reviewed and certify the information provided above is true and correct to the best of my knowledge. I will notify MHCP Provider Enrollment of any additions or changes to the information. By signing this form, I acknowledge I have read and understand the Application and Background Study Privacy Notice. I also authorize MHCP to use the information collected about me according to the Privacy Notice. NAME OF INDIVIDUAL SUPPORT WORKER (PRINT OR TYPE) SIGNATURE OF INDIVIDUAL SUPPORT WORKER DATE SIGNED Agency Information AGENCY NAME AGENCY NPI/UMPI AGENCY FAX NUMBER AGENCY PERSONNEL COMPLETING FORM AGENCY PERSONNEL SIGNATURE Next Steps Read, sign and date the MHCP Provider Agreement - Support Worker (CDCS, CSG, PCA) (DHS-4611), and return it with this application. Fax both the application and agreement to MHCP will process only completed fax requests.
4
5 *DHS-4611-ENG* DHS-4611-ENG 4-15 Minnesota Health Care Programs Provider Agreement Individual Support Worker (CDCS, CSG, PCA) As a participating provider in health service programs administered by the Minnesota Department of Human Services (the Department), the Provider agrees to: A. Submit documentation to your affiliated agency that fully discloses the extent of services provided to individuals under these programs. The documentation must be legible and meet the requirements of Minnesota Statutes Section 256B.0659, subdivision 12 for all individual support workers in CDCS, CSG, and PCA. B. Furnish the Department, the Secretary of the U.S. Department of Health and Human Services (DHHS), or the Minnesota Medicaid Fraud Control Unit with such information as it may request regarding payments claimed for services provided under these programs. C. Comply with all federal and state statutes and rules relating to the delivery of services to individuals and to the submission of claims for such services. D. Accept as payment in full, amounts paid in accordance with schedules established by the Department, except where payment by the recipient has been authorized by the Department. E. Make full disclosure of any convictions(s) of program crimes as required by 42 C.F.R F. Comply with all federal statutes, implementing regulations and guidance prohibiting discrimination on the basis of race, color, national origin, sex, age, religion and disability in any program or activity receiving federal financial assistance from DHHS; and to comply with the Minnesota Human Rights Act. G. Render to recipients services of the same scope and quality as would be provided to the general public, within Minnesota Health Care Programs (MHCP) guidelines. H. Comply with the provisions of any fully executed agreement and/or addendum required by the Department, which is incorporated herein by reference. I. Comply with the advance directive requirements as required by 42 C.F.R and J. Properly handle and safeguard protected information collected, created, used, maintained, or disclosed on behalf of the Department. For purposes of this Agreement, protected information means data subject to any of the following laws: 1. The Minnesota Government Data Practices Act (MGDPA), Minnesota Statutes Chapter 13, in particular ( welfare data ); 2. The Minnesota Health Records Act and ; 3. The Health Insurance Portability and Accountability Act ( HIPAA ), including but not limited to the requirements of the Privacy Rule and the Security Regulations, 45 C.F.R. Part 160 and Part 164, subparts A and E. 4. Federal law and regulations that govern the use and disclosure of substance abuse treatment records, 42 U.S.C.S. 290dd-2 and 42 C.F.R. 2.1 to 2.67; and 5. Any other applicable state and federal statutes, rules, and regulations affecting the collection, storage, use and dissemination of private or confidential information. DIRECT SUPPORT WORKER INITIALS NAME OF SUPPORT WORKER UMPI Page 1 of 3
6 K. Comply with the laws described in section J. This includes the Provider: 1. Not using or further disclosing protected information created, collected, received, stored, used, maintained or disseminated in the course or performance of this Agreement other than as necessary to perform its obligations under this Agreement, or as required by law, either during the period of this Agreement or hereafter. See, respectively, 45 C.F.R (b) and (d), and Minn. Stats subd Using appropriate administrative, physical, and technical safeguards to prevent use or disclosure of the protected information other than as provided for by this Agreement and to ensure the confidentiality, integrity, and availability of any electronic protected health information (PHI) that it creates, receives, maintains, or transmits on behalf of the Department. Provider will not transmit PHI over the Internet or any other unsecure or open communications channel unless such information is encrypted or otherwise safeguarded using procedures no less stringent than those described in 45 C.F.R If the Provider stores or maintains PHI in encrypted form, the provider shall, at the Department s request, promptly provide the Department with the key or keys to decrypt such information. The Provider shall not forward previously encrypted data to any other party, unless otherwise required by this Agreement. 3. Mitigating, to the extent practicable, any harmful effects known to the Provider of a use, disclosure, or breach of security with respect to protected information by the Provider in violation of this Agreement. L. Agree that this Agreement may be immediately terminated at the discretion of the Department if it determines that the Provider has violated a material term of the Agreement, including but not limited to, non-compliance by the Provider with the HIPAA Privacy Rule and Security Standards. If termination is not feasible, the Department shall report the breach to the Secretary of DHHS. Upon termination of this Agreement, all of the protected information provided by the Department to Provider, or created or received by the Provider on behalf of the Department, that the Provider still maintains in any form, including information that is in the hands of subcontractors or agents of the Provider, shall be destroyed or returned to the Department, and the Provider shall retain no copies of such information. If it is infeasible to return or destroy the information, the Provider shall provide the Department notification of the conditions that make return or destruction infeasible, and shall extend the protections of this Agreement to such information and limit further use and disclosure of such information to those purposes that make return or destruction infeasible, for as long as the Provider maintains the information. M. Agree that any ambiguity in this Agreement shall be resolved to permit the Department to comply with HIPAA, MDGPA, and other applicable state and federal statutes, rules, and regulations affecting the collection, storage, use and dissemination of private or confidential information and other state and federal laws and regulations. Upon signature, this Provider Agreement supersedes and replaces all former Provider Agreements the Provider has with the Department. An individual applicant must personally sign the Provider Agreement. Please sign and date below, initial page 1, and return both page 1 and page 2 of this agreement. Please retain a copy of the provider agreement for your files, and return the original to the Department of Human Services. NAME OF SUPPORT WORKER (TYPE OR PRINT) TITLE SIGNATURE OF SUPPORT WORKER DATE Please return page 1 and page 2 of this document Page 2 of 3 DHS-4611-ENG 4-15
7 Agreement Summary As an individual support worker, you are providing health care services to individuals. We require your enrollment in the Minnesota Health Care Programs (MHCP) so that you are represented on the claim as the person who provided the services. Knowing that a qualified individual provided the service ensures the safety of the people that the Minnesota Department of Human Services serves. It also allows the Department to perform auditing and tracking of services which protects against double-billing and other types of fraud. Before enrollment is approved, MHCP must make certain that: 1. There is no legal or other reason why you shouldn t provide these services, 2. You understand what is necessary to properly provide these services, and 3. You understand the need to protect the privacy of the people you care for. To help ensure that each of these conditions is met, MHCP requires that you agree to the terms in the attached Provider Agreement. In general, this agreement requires that you: A. Provide documents to your employer about the services you provide. B. Provide documents to MHCP or other state and federal agencies related to the services you provide, when requested. C. Comply with federal and state laws about the services you provide. D. Accept payment made to your employer as payment in full for the services you provide. You cannot ask for nor accept additional payment from the client. E. Disclose any criminal convictions you have related to Medicare, Medicaid, or title XX services. F. Not discriminate against individuals because of their race, color, national origin, sex, age, religion or disability when you provide these services. G. Provide the same quality of service to persons receiving public assistance as those who don t receive such assistance. H. If you are enrolled to provide and bill for other services, you must continue to follow the requirements of the agreement you signed when you enrolled for those services. The terms of that agreement are different than the terms in the attached agreement. I. Comply with federal requirements about advance directives. An advance directive is written instruction, such as a living will, to give a patient control over medical treatment decisions. J. Properly protect private information about the people to whom you provide services, especially their health information. K. Don t disclose the private information of someone for whom you provide services, unless it is needed for your work. This includes not discussing someone s private information unless your job requires it. Also, ensure that the information could not be accessed by someone who does not have permission to see it. This includes not leaving paperwork out where others can see it, and not sending private information over the internet. L. Understand that this agreement may be canceled if you violate its terms. If this agreement is canceled, you must properly dispose of any private information you have about the people you serve so that it is not discovered by someone who does not have permission to see it. M. Understand that by signing this agreement, you are agreeing to protect any private information you come in contact with in your job. When you protect private information, you are complying with federal and state laws, and you help the Department comply with these laws, as well. This is a basic description of the terms of this agreement. By signing this agreement, you are agreeing to be legally bound by all of its terms. If you have questions about it, you should get answers to them before signing this agreement. If you need or want legal advice, you should contact your own attorney. For more information, please call Page 3 of 3 DHS-4611-ENG 4-15
8
9 Request for Background Study Form For CSG Only Background studies for CSG Workers under the Payroll Model are OPTIONAL and conducted only at the request of the Representative. If you DO want PICS to process a background study on the Worker: 1. Representative completes this Request for Background Study Form. 2. Worker completes the Background Study Authorization Form (see next page). Worker Name: Representative Name: As the Representative, I authorize Partners in Community Supports (PICS) to process a Criminal Background Study on my Worker through Worker Signature Date Representative Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
10
11 Background Study Authorization Please Note: Background study results must be complete within Minnesota Statute 245c.14 before providing direct support. Personal Supports/CDCS program - Processed through MN Department of Human Services and fingerprinting is required. CSG program - Processed through backgroundchecks.com and fingerprinting is not required. Background Study Instructions Worker submits Background Study Form and copy of photo ID PICS submits Worker's information to DHS. PICS sends Fingerprinting Instructions to Worker. Worker completes fingerprinting at approved location. PICS receives background study results within 3 business days. Worker Information (submit form with copy of photo ID) FIRST NAME MIDDLE NAME (FULL) LAST NAME (LEGAL) DATE OF BIRTH GENDER DRIVER S LICENSE/STATE ID # STREET ADDRESS CITY STATE ZIP CODE PHONE NUMBER RACE PLACE OF BIRTH (STATE or COUNTRY) SOCIAL SECURITY NUMBER PRIOR NAMES AND ALIASES USED Required if you have lived outside of Minnesota in the last 5 years. CITY STATE YEAR YEAR AT ADDRESS Required If photo ID doesn t include eye color, hair color, height, and weight. EYE COLOR HAIR COLOR HEIGHT COUNTY WEIGHT I authorize PICS to conduct a background study for the purpose of evaluating my potential employment with PICS. I verify that all the above information is correct to the best of my knowledge. Worker Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
12 Acceptable Forms of Identification For DHS Background Studies Entities that initiate background studies are required by law to verify the background study subject s identity in NETStudy 2.0. This is a summary of acceptable forms of identification to be used for DHS background studies. Primary Identification Document When a background study subject has a valid* picture identification listed below use this document for identity verification: State-Issued Driver s License the issuing authority must be a US state or territory State-Issued Identification Card the issuing authority must be a US state or territory US Passport or US Passport Card *Valid Documentation: Only unexpired, original documentation is acceptable, except when a background study subject presents an acceptable receipt for a primary or secondary identification document. There are three types of acceptable receipts: A receipt showing that the subject has applied to replace the primary or secondary identification document; The arrival portion of Form I-94/I-94A with a temporary I-551 stamp and photograph of the individual; The departure portion of Form I-94/I-94A with a refugee admission stamp. Secondary Identification Document If a background study subject does not have a valid picture identification listed above, the following secondary identification documents (consistent with federal employment requirements and the I9 form) may be used for identity verification: School ID card that includes a photograph Voter s registration card US military card or draft record Military dependent s ID card US Coast Guard Merchant Mariners Document (MMD) Card Native American tribal document Driver s License issued by a Canadian government authority Permanent Resident Card or Alien Registration Receipt Card (Form I-551) Foreign passport containing temporary I-551 stamp/printed notation on a machine-readable immigrant visa (MRIV) Employment Authorization Document (Card) that contains a photograph (Form I-766) Foreign passport with Form I-94/I-94A, Arrival/Departure Report bearing the same name as the passport and containing an endorsement of the alien s nonimmigrant status that authorizes such alien to work for a specific employer incident to this status. This document may only be used if the period of endorsement has not yet expired. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94/I- 94A showing nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI. Foreign passport with special documents issued by the Commonwealth of Northern Mariana Islands (CNMI) Foreign passport that contains a temporary I-551 stamp/printed notation on a machine-readable immigrant visa (MRIV) Exceptions People Under Age 18 People under 18 who are unable to present a picture identification document listed in the Primary Identification Document section may present the following acceptable secondary identification documents: School report or report card Clinic, doctor, or hospital record Day-care, or nursery school record Legal References Information required to be provided by background study subjects; See Minnesota Statutes, section 245C.05, subd. 1. Information required to be verified by the entity initiating the background study; See Minnesota the issuing authority must be a US state or territory; See Minnesota Statutes, section 245C.05, subd. 2 (a). hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
13 BACKGROUND STUDY NOTICE OF PRIVACY PRACTICES Because the Department of Human Services (DHS) is asking you to provide private information, you have privacy rights under the Minnesota Government Data Practices Act. This law protects your privacy, but also allows DHS to give information about you to others when the law requires it. This notice describes how your private information may be used and disclosed, and how you may access your information. Why is DHS asking me for my private information? A background study from the Department of Human Services (DHS) is required for your job or position. The private information is needed to conduct the background study. How will I be notified that a background study was submitted on me? DHS will mail you a notice within three working days after a request for a background study is submitted on you. The notice will contain the background study result or let you know that more time is needed to complete the background study. The notice will also identify the entity that submitted the background study request. What information must I provide to complete the background study? You are required to provide enough information to ensure an accurate and complete background study. This includes your: first, middle, and last name and all names you have ever been known by or used; current home address, city, zip code, and state of residence; previous home addresses, city, county, and states of residence for the last five years; sex and date of birth; driver s license or other identification number, and; fingerprints and a photograph. How will the information that I give be used? The information will be used to perform a background study that will include a check to determine whether you have any criminal records and/or have been found responsible for substantiated maltreatment of a vulnerable adult or child. Background study data is classified as private data and cannot be shared without your consent except as explained in this notice. What may happen if I provide the information? You could be disqualified from positions that require a DHS background study if you are found to have committed certain crimes, been determined responsible for maltreatment of a vulnerable adult or child, or have other records that require a disqualification. If you do not have a disqualifying record, you will be cleared to work. -1- What if I refuse to provide the information? You will be disqualified if you refuse to provide information to complete an accurate background study. You will not be able to work in a position that requires a DHS background study. Who will DHS give my information to? DHS will only share information about you as needed and as allowed or required by law. The identifying information you provide will be shared with the Minnesota Bureau of Criminal Apprehension and in some cases the Federal Bureau of Investigation (FBI). If there is reasonable cause to believe that other agencies may have information related to a disqualification, your identifying information may also be shared with: county attorneys, sheriffs, and agencies; courts and juvenile courts; local police; the Office of the Attorney General, and; agencies with criminal record information systems in other states. What information will DHS share with the entity that requested my background study? The entity that requested the background study will be notified of your background study determination. If you are disqualified, the entity will not be told the reason unless you were disqualified for refusing to cooperate with the background study or for substantiated maltreatment of a minor or vulnerable adult. What other entities might DHS share information with? Information about your Background study may be shared with: the Minnesota Department of Health; the Minnesota Department of Corrections; the Office of the Attorney General, and; health-related licensing boards.
14 What if my disqualification is set aside? If you request reconsideration of your disqualification and your disqualification is set aside, the entity that requested the background study will be informed of the reason(s) for your disqualification unless the law states otherwise. DHS will provide information about the decision to set aside your disqualification if the entity requests it. Unless prohibited by law, your name and the reason(s) for your disqualification will become public data if your set aside is for: a child care center or a family child care provider licensed under chapter 245A, or; an offense identified in section 245C.15, subdivision 2. For future background studies submitted by entities that provide the same type of services as the services you were set aside for, the set aside will apply unless: you were disqualified for an offense in section 245C.15, subdivision 1 or 2, or; DHS receives additional information indicating that you pose a risk of harm, or; your set aside was limited to a specific person receiving services. In addition, those entities will be informed of the reason(s) for your disqualification unless prohibited by law. Will my fingerprints be kept? DHS and the Bureau of Criminal Apprehension will not keep your fingerprints. However, if an FBI check is required for your background study, the Federal Bureau of Investigation (FBI) will keep your fingerprints and may use them for other purposes. What information can the fingerprint and photo site view and keep? The fingerprint and photo site can view identifying information to verify your identify. The fingerprint and photo site will not keep your fingerprints, photo, or most other information. The fingerprint and photo site can keep your name and the date and time your fingerprints were recorded and sent, for auditing and billing purposes. Who can see my photo? Your photo will be kept by DHS. If you provide your social security number to allow your background study to be transferable to future entities, your photo will be available to those entities to verify your identity. What are my rights about the information you have about me? You may ask if we have information about you and request in writing to get copies. You may have to pay for copies. You may give other people permission to see and have copies of private information about you. You may ask in writing a report that lists the entities that submitted a background study request on you. You may ask in writing that the information used to complete your background study be destroyed. The information will be destroyed if you have: (1) not been affiliated with any entity for the previous two years, and; (2) no current disqualifying characteristic(s). Please send all written requests to: Minnesota Department of Human Services Background Studies Division NETStudy 2.0 Coordinator PO Box St. Paul, MN How long will DHS keep my background study information? DHS will destroy: your photo when you have not been affiliated with an entity for two years. any background data collected on a you after two years following your death or 90 years after your date of birth, except when readily available data indicates that you are still living. What is the legal authority for DHS to conduct background studies? Background studies are completed by DHS according to the requirements in Minnesota Statutes, chapter 245C. Background studies are authorized under Minnesota Statutes, sections 256B.0943, subdivision 5a; 256B.0659, subdivision 11(a)(3); , subdivision 6(a); , subdivision 1; , subdivision 4, and ; What if I think my privacy rights have been violated? You may report a complaint if you believe your privacy rights have been violated. If you think that the Minnesota Department of Human Services violated your privacy rights, you may send a written complaint to the Minnesota Department of Human Services, Privacy Official at: Minnesota Department of Human Services Privacy Official PO Box St. Paul, MN Updated: 02/12/2015
15 Personnel File Notification Workers rights and remedies regarding review of personnel file under PICS policies and in compliance with Minnesota state law. Worker Name: A. Review of Personnel File How: Workers may make a written request to the Human Resources Department to review their personnel file; however, such requests may be limited to no more than once every six months and may be denied if we determined that the request was not made in good faith. Upon separation from employment a former worker may make such a written request once each year after separation for as long as the personnel record is maintained. When: Upon receipt of a written request from a worker or former worker to review their personnel file it is our practice to comply no later than 7 working days. What: Arrangements will be made for current workers to inspect their personnel record during normal business hours. An accurate copy of the personnel file may be used or simply provided; a copy will be mailed to any former worker at an address disclosed in a written request and onsite inspections will not be allowed for former workers. B. Removal or Revision of Personnel File Information If a worker disputes any of the specific information contained in their personnel file, there are three different courses of action that may be taken: 1. Worker may do nothing about the disagreement; 2. Worker may seek management s agreement to revise/remove disputed information, which may or may not be granted; and 3. If no agreement is reached to revise or remove the disputed information, the worker may submit a written statement specifically identifying the disputed information and explaining their position on the information in question. This position statement may be no longer than 5 written pages and will be included with worker s personnel file with the disputed information, for as long as the disputed information is contained in the record. C. Worker Records Our employment records also require that contract and other information be maintained current and updated as needed. Workers are responsible for notifying the Human Resource Generalist promptly and accurately in writing of any changes relating to personal information, such as home address, telephone number, marital status, and/or number of dependents. D. Remedies/Retaliation Prohibited In addition to other remedies provided by law, if any, worker may bring a civil action in an attempt to compel compliance with these provisions regarding their right to inspect his or her personnel file and potentially seeking the following relief: 1. Actual damages only, plus costs, under Minn. Stats to ; and 2. Actual damages, back pay, and reinstatement or other make-whole equitable relief, plus reasonable attorney s fees, under Minn. Stat Any worker who in good faith exercises their rights and remedies regarding review of the personnel record under these provisions may not be retaliated against. Acknowledgement of Receipt I hereby acknowledge that I have received a copy of the foregoing Personnel File Notification and I understand that I am obligated to read and familiarize myself with its terms. Worker Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
16

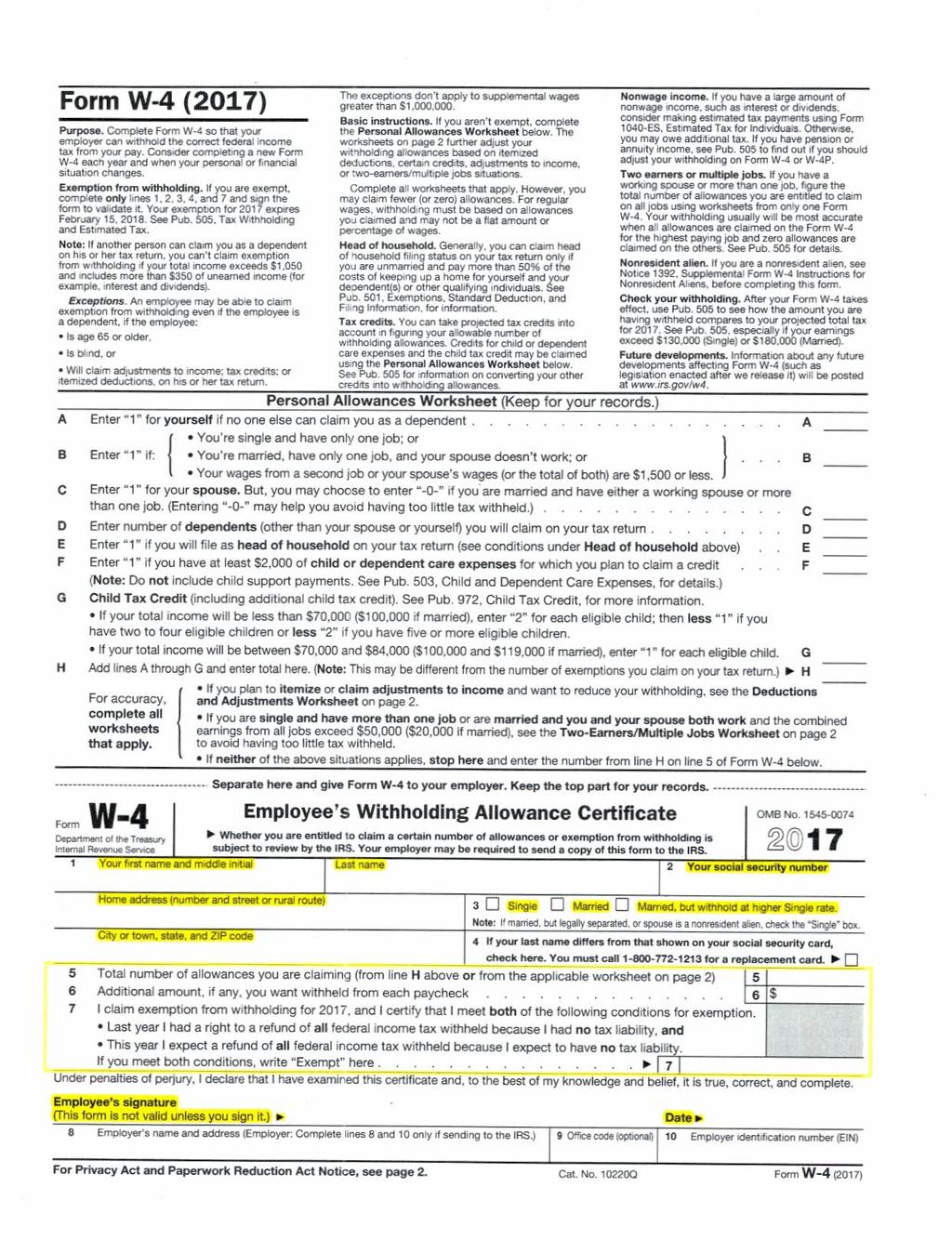
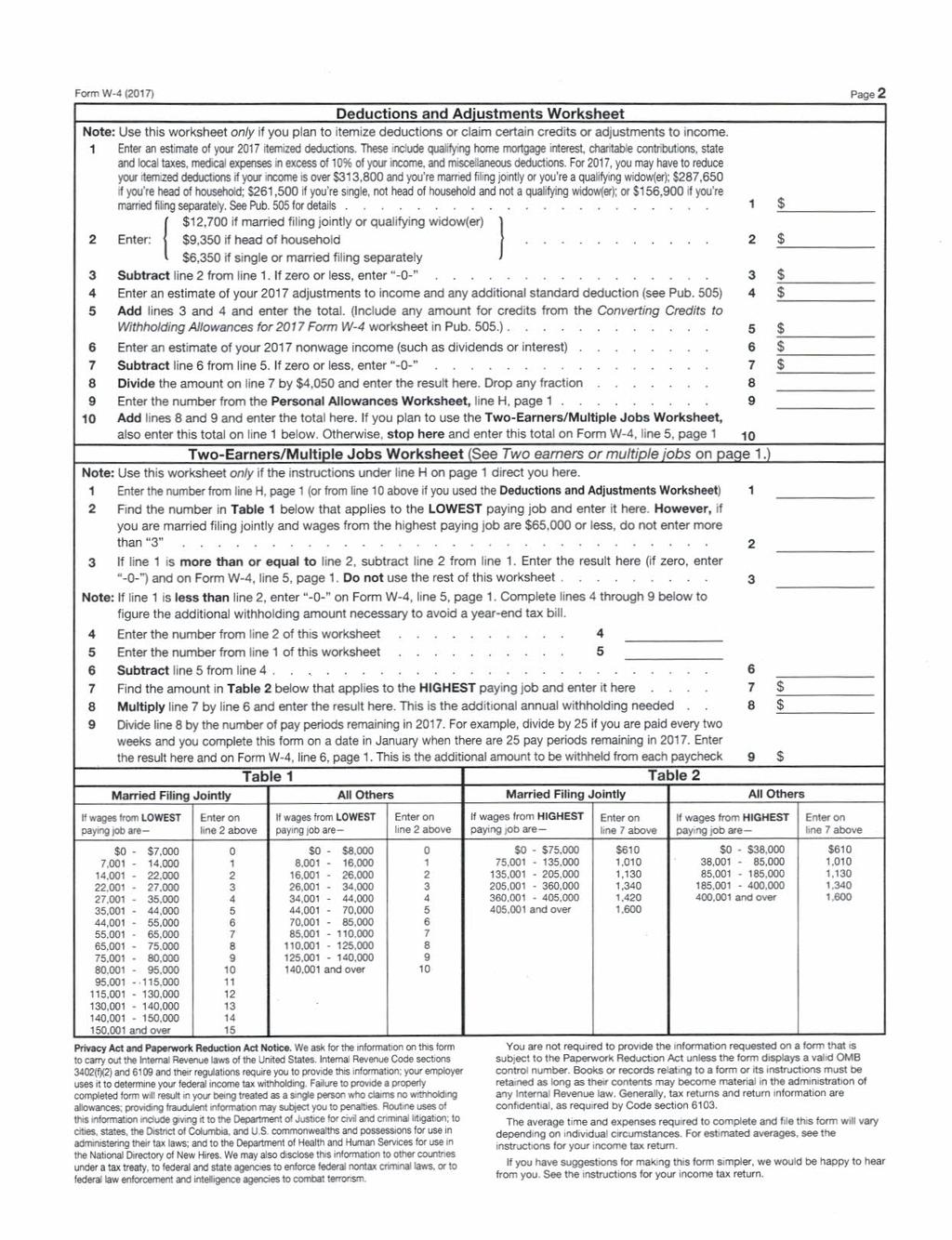
17 Federal W-4 Form Sample Purpose of this Form: To tell PICS the correct federal income tax withholdings to withhold from your paycheck. If form is incomplete by your first paycheck, you will be set up as default tax status of Single and Zero. Based on Tax Determination, You Must Write: Allowance amount on Line 5 OR The word exempt on Line 7. Line 7 only applies if you are eligible for exemption. If Claiming Exempt: If claiming exempt on Line 7, you MUST complete a new Federal W-4 form and State W-4 form. Must provide PICS with a new Federal W-4 Form and State W-4 form by February 15 th each year. Please Note: Cannot complete both Line 5 AND Line 7. Federal W-4 Form is revised once a year. PICS cannot accept expired federal forms. PICS is not a tax consultant. To verify tax status, please consult your tax professional. hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
18
19
20
21 Payment Options Form Partners in Community Supports (PICS) requires electronic payment for payroll. Please complete this form and return to PICS before submitting your first timesheet. Worker Name: Street Address: City: State: Zip Code: Phone Number: Date of Birth: / / Social Security # (last 4 Digits): Please choose Option 1 or Option 2 - *A debit card will be issued if form is not completed.* See back page for more details. OPTION 1 - Direct Deposit Choose up to 2 accounts. The 2nd account is for the remaining amount. A bank document must be submitted along with this form. It must show your name, bank s name, routing number, and account number. You can submit a voided check, bank statement, or typed bank letter. 1. Bank Name: 2. Bank Name: Routing Number: Routing Number: Account Number: Account Number: Savings Amount to Deposit: $ or Entire Check Account Type: Checking Account Type: Checking Savings * I authorize Partners in Community Supports ( Company ) to deposit any amounts owed me by initiating credit entries to my accounts at the financial institutions ( Bank ) indicated on this form. I authorize Bank to accept and credit any credit entries indicated by Company to my accounts. In the event that Company deposits funds erroneously into my account, I must provide written consent to authorize Company to debit my account for an amount not to exceed the original amount of the erroneous credit. This authorization is to remain in full force and effect until Company and Bank have received written notice from me of its termination in such time and manner as to afford Company and Bank reasonable opportunity to act on it. OPTION 2 - Payroll Debit Card PICS will issue and mail to you a payroll debit card. Your pay will be deposited into the TotalPay Card and Money Network Check Program account every payday. * I authorize my employer, as well as any payroll services provider authorized by my employer, to initiate credit entries. In the event that Company deposits funds erroneously into my account, I must provide written consent to authorize Company to debit my account for an amount not to exceed the original amount of the erroneous credit. Worker Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
22 OPTION 1 - Direct Deposit Additional Information for Payment Options To enroll in Direct Deposit, complete form on the front side with your account information and return it to PICS along with a bank document that includes: your name the bank s name routing number account number This bank document must come directly from the bank and must be computer generated. It can be a: voided check bank statement typed letter from the bank Deposit Slips are NOT accepted. OPTION 2 - Payroll Debit Card ADP TotalPay Visa Debit Card and Money Network Checks To receive a TotalPay Debit Card, complete form on the front side and return to PICS. PICS will issue and mail the debit card to you before your first pay check. Upon receipt, you will activate the card and begin to use the benefits of the TotalPay Debit Card. The TotalPay Card and Money Network Checks offer you a complete and convenient package of services you can use to access and manage your money instantly. Your pay will be deposited into the TotalPay Card and Money Network Check Program Account ( Account ) every payday so you have immediate access to your money. Advantages to TotalPay Check account balance for free online or by phone Pay bills online with TotalPay Card Manage account online or by phone Get cash at an ATM Use a Money Network Check Make purchases hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017

23 I-9 Form Sample If the I-9 form does not meet Homeland Security requirements, it is considered invalid. PICS Human Resources will request the completion of a new form. The Federal Instructions are available on our website. Front Page: Worker will complete steps 1-3. Please note that you cannot use an electronic signature on the I-9 form. hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017


24 Back Page: Representative or Authorized Representative will complete steps 1-3 on the back page. The Authorized Representative can be a non-relative or notary. The Employer s Business Name will be the FEIN Holder s Name and the Employer s Business Address will be the FEIN Holder s home address. Please note that you cannot use an electronic signature on the I-9 form. *The Worker CANNOT complete the back page of their own I-9 form.* hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
25 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination. Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.) Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any) Address (Street Number and Name) Apt. Number City or Town State ZIP Code Date of Birth (mm/dd/yyyy) U.S. Social Security Number - - Employee's Address Employee's Telephone Number I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form. I attest, under penalty of perjury, that I am (check one of the following boxes): 1. A citizen of the United States 2. A noncitizen national of the United States (See instructions) 3. A lawful permanent resident (Alien Registration Number/USCIS Number): 4. An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy): Some aliens may write "N/A" in the expiration date field. (See instructions) Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number. QR Code - Section 1 Do Not Write In This Space 1. Alien Registration Number/USCIS Number: OR 2. Form I-94 Admission Number: OR 3. Foreign Passport Number: Country of Issuance: Signature of Employee Today's Date (mm/dd/yyyy) Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1. (Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.) I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct. Signature of Preparer or Translator Today's Date (mm/dd/yyyy) Last Name (Family Name) First Name (Given Name) Address (Street Number and Name) City or Town State ZIP Code Employer Completes Next Page Form I-9 07/17/17 N Page 1 of 3

26 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No Expires 08/31/2019 Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.") Employee Info from Section 1 Last Name (Family Name) First Name (Given Name) M.I. Citizenship/Immigration Status List A OR List B AND List C Identity and Employment Authorization Identity Employment Authorization Document Title Document Title Document Title Issuing Authority Document Number Issuing Authority Document Number Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space Expiration Date (if any)(mm/dd/yyyy) Document Title Issuing Authority Document Number Expiration Date (if any)(mm/dd/yyyy) Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions) Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.) A. New Name (if applicable) B. Date of Rehire (if applicable) Last Name (Family Name) First Name (Given Name) Middle Initial Date (mm/dd/yyyy) C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below. Document Title Document Number Expiration Date (if any) (mm/dd/yyyy) I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative Form I-9 07/17/17 N Page 2 of 3
27 LISTS OF ACCEPTABLE DOCUMENTS All documents must be UNEXPIRED Employees may present one selection from List A or a combination of one selection from List B and one selection from List C. LIST A Documents that Establish Both Identity and Employment Authorization LIST C Documents that Establish Employment Authorization OR LIST B Documents that Establish Identity AND 1. U.S. Passport or U.S. Passport Card 2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551) 3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machinereadable immigrant visa 4. Employment Authorization Document that contains a photograph (Form I-766) 5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status: a. Foreign passport; and b. Form I-94 or Form I-94A that has the following: (1) The same name as the passport; and (2) An endorsement of the alien's nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form. 6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI 1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address 3. School ID card with a photograph 4. Voter's registration card 5. U.S. Military card or draft record 6. Military dependent's ID card 7. U.S. Coast Guard Merchant Mariner Card 8. Native American tribal document 9. Driver's license issued by a Canadian government authority For persons under age 18 who are unable to present a document listed above: 10. School record or report card 11. Clinic, doctor, or hospital record 12. Day-care or nursery school record 1. A Social Security Account Number card, unless the card includes one of the following restrictions: (1) NOT VALID FOR EMPLOYMENT (2) VALID FOR WORK ONLY WITH INS AUTHORIZATION (3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION 2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240) 3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal 4. Native American tribal document 5. U.S. Citizen ID Card (Form I-197) 6. Identification Card for Use of Resident Citizen in the United States (Form I-179) 7. Employment authorization document issued by the Department of Homeland Security Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274). Refer to the instructions for more information about acceptable receipts. Form I-9 07/17/17 N Page 3 of 3
28
29 FEIN Questionnaire Participant Employer Information Participant Employer Name: FEIN #: - MN Revenue ID #: Participant Name: Representative Name: Worker Information Worker Name: Date of Birth: / / Job Title: Direct Support Professional Homemaker Work Schedule: Part-Time (29 hours or less per week) Full-Time (30 hours or more per week) Wage Rate: $ per hour Type: Staffing Respite Homemaker Other: $ per hour Type: Staffing Respite Homemaker Other: Relationship to Participant: Parent Spouse Legal Guardian Sibling No Relation Other: Indicate Worker s relationship to Participant Employer: Income FUTA SUTA Workers FICA Relationship to Tax Compensation Participant Employer Federal/ State Medicare/ Social Security Federal Unemployment State Unemployment Parent/Stepparent EXEMPT EXEMPT EXEMPT not required Spouse EXEMPT EXEMPT EXEMPT not required *Legal Guardian Based TAXABLE TAXABLE TAXABLE required Child/Stepchild: Age on W-4 EXEMPT EXEMPT TAXABLE required Minors: Age EXEMPT EXEMPT EXEMPT required *General Household Worker: Age 18 EXEMPT TAXABLE TAXABLE required *General Household Worker: Age 19 or older TAXABLE TAXABLE TAXABLE required *Legal Guardians must provide legal documentation proving legal guardianship. *General Household Worker includes siblings, children (age 22 or older), grandparents, cousins, and Workers with no relation. I hereby certify that the information above is true and accurate. Worker Signature Date Representative Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
30
31 Employment Application Personal Information Worker Name: Phone: Years of Related Experience to Direct Support: Less than 5 5 or more Street Address: City/State/Zip: Primary Language: Emergency Contact Name: Emergency Phone Number: Education and Training School Level Name and Location Graduated? Degree Received High School Yes No College Other Relevant License or Certification Title Yes No Yes No Effective Dates Employment History Company Name: Dates of Employment: Title: Reason for Leaving: Ending Salary or Hourly Rate: $ Supervisor Name: May we contact your supervisor? Yes No Supervisor Phone Number: Company Name: Dates of Employment: Title: Reason for Leaving: Ending Salary or Hourly Rate: $ Supervisor Name: May we contact your supervisor? Yes No Supervisor Phone Number: Professional References Name: Relation: Phone Number: Name: Relation: Phone Number: I certify that the information on this application is true and accurate. I realize that any false or incomplete information may result in rejection of this application, refusal to hire, or immediate discharge. I understand that Partners in Community Supports (PICS) is an Equal Opportunity Employer. I understand that this application is not a contract for employment I may resign at any time for any reason and PICS may terminate my employment at any time for any legal reason. Worker Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
32
33 Job Description The Representative establishes the job duties based on the needs of the Participant and objective of the Participant s County Plan. This job description may be amended periodically by the Representative and will be provided to the Worker. Worker Name: Participant Name: Job Title: Direct Support Professional Homemaker Work Schedule: Part-Time (29 hours or less per week) Full-Time (30 hours or more per week) Responsibilities - Indicate level of job duties for each category required to perform for Participant. Dressing Full Assistance Partial Assistance Verbal Prompts Not Applicable Recreation Full Assistance Partial Assistance Verbal Prompts Not Applicable Transportation Full Assistance Partial Assistance Verbal Prompts Not Applicable Correspondence Full Assistance Partial Assistance Verbal Prompts Not Applicable Shopping Full Assistance Partial Assistance Verbal Prompts Not Applicable Bathroom Full Assistance Partial Assistance Verbal Prompts Not Applicable Housekeeping Full Assistance Partial Assistance Verbal Prompts Not Applicable Meal Prep Full Assistance Partial Assistance Verbal Prompts Not Applicable Exercise Full Assistance Partial Assistance Verbal Prompts Not Applicable Other: *Full Assistance - Completes activity for client. *Verbal Prompts - Gives verbal reminders to client. *Partial Assistance - Helps client with activity. *Not Applicable - Client doesn t need assistance. I have reviewed and agree to the responsibilities of the job. Worker Signature Date Representative Signature Date hr@picsmn.org Phone: Fax: Eustis Street, St. Paul, MN Copyright PICS Partners in Community Supports, 2017
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Last Name First name Middle Initial Address DETACH HERE
 Centralized Employee Registry Reporting Form To be completed by the employer within 15 days of hire. Please print or type. EMPLOYER INFORMATION FEIN Required - - FEIN plus last 3-digit suffix used when
Centralized Employee Registry Reporting Form To be completed by the employer within 15 days of hire. Please print or type. EMPLOYER INFORMATION FEIN Required - - FEIN plus last 3-digit suffix used when
EMPLOYEE UPDATE FORM
 EMPLOYEE UPDATE FORM Date Submitted: First Name M.I. Last Name Address City State Zip County SSN DOB E-Mail Hire Date: Termination Date: Change Date: Auth. Signature Marital Status: Married Single Gender:
EMPLOYEE UPDATE FORM Date Submitted: First Name M.I. Last Name Address City State Zip County SSN DOB E-Mail Hire Date: Termination Date: Change Date: Auth. Signature Marital Status: Married Single Gender:
LOAN-OUT COMPANY START FORM AND AGREEMENT
 150 West 30th Street, Suite 405 New York, NY 10001 (212) 206-1724 tel. (212) 206-1070 fax LOAN-OUT COMPANY START FORM AND AGREEMENT Production Company Loaned Out Employee Name Production Title Name of
150 West 30th Street, Suite 405 New York, NY 10001 (212) 206-1724 tel. (212) 206-1070 fax LOAN-OUT COMPANY START FORM AND AGREEMENT Production Company Loaned Out Employee Name Production Title Name of
International Student Employment Packet
 International Student Employment Packet Most commonly provided items to bring to the Financial Aid Office: I-94 I-20 or DS-2019 Unexpired Foreign Passport Receipt of application for Social Security Card
International Student Employment Packet Most commonly provided items to bring to the Financial Aid Office: I-94 I-20 or DS-2019 Unexpired Foreign Passport Receipt of application for Social Security Card
EMPLOYEE PAYROLL ENROLLMENT AND UPDATE FORM
 EMPLOYEE PAYROLL ENROLLMENT AND UPDATE FORM Employer Date Submitted: First Name M.I. Last Name Address City State Zip County SSN DOB E-Mail Hire Date: Termination Date: Change Date: Auth. Signature Marital
EMPLOYEE PAYROLL ENROLLMENT AND UPDATE FORM Employer Date Submitted: First Name M.I. Last Name Address City State Zip County SSN DOB E-Mail Hire Date: Termination Date: Change Date: Auth. Signature Marital
NEW HIRE / REPLACEMENT INFORMATION
 NEW HIRE / REPLACEMENT INFORMATION NAME: ADDRESS: CITY, STATE, & ZIP: SOCIAL SECURITY #: DATE OF BIRTH: LOCAL NUMBER FILING STATUS: SINGLE OR MARRIED - PLEASE CIRCLE ONE NUMBER OF DEPENDENTS: CLASS: (1
NEW HIRE / REPLACEMENT INFORMATION NAME: ADDRESS: CITY, STATE, & ZIP: SOCIAL SECURITY #: DATE OF BIRTH: LOCAL NUMBER FILING STATUS: SINGLE OR MARRIED - PLEASE CIRCLE ONE NUMBER OF DEPENDENTS: CLASS: (1
Instructions for Remote Workers on Completing the Form I-9 Employment Verification
 Instructions for Remote Workers on Completing the Form I-9 Employment Verification Federal Law requires that Carnegie Mellon University must have a valid Form I-9 on file for every employee. Federal Law
Instructions for Remote Workers on Completing the Form I-9 Employment Verification Federal Law requires that Carnegie Mellon University must have a valid Form I-9 on file for every employee. Federal Law
Are you a current WVU student? (Circle One)
") \X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: Legal First
\X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: Legal First
Are you a current WVU student? (Circle One)
") \X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: First Name
\X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: First Name
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Student Employee New-Hire Paperwork
 Student Employee New-Hire Paperwork Congrats on landing your first on campus job! In order to be hired and paid on time, you must complete the new hire process by following steps 1-6 outlined below. E-Verify
Student Employee New-Hire Paperwork Congrats on landing your first on campus job! In order to be hired and paid on time, you must complete the new hire process by following steps 1-6 outlined below. E-Verify
Employment Application An Equal Opportunity Employer
 Employment Application An Equal Opportunity Employer AllianceHR New Hire Policy: Prior to the employee starting work, the Employee Application and the Employment Eligibility Form (I-9) must be completed
Employment Application An Equal Opportunity Employer AllianceHR New Hire Policy: Prior to the employee starting work, the Employee Application and the Employment Eligibility Form (I-9) must be completed
Form I9 Employment Eligibility Verifications
 Form I9 Employment Eligibility Verifications 1. Purpose of document: To document verification of the identity and employment authorization of each new employee (both citizen and noncitizen) hired after
Form I9 Employment Eligibility Verifications 1. Purpose of document: To document verification of the identity and employment authorization of each new employee (both citizen and noncitizen) hired after
APPLICATION FOR SUPPORT PERSONNEL PLEASE READ THIS INSTRUCTION SHEET CAREFULLY
 VERNON PARISH SCHOOL SYSTEM 201 BELVIEW ROAD LEESVILLE, LA 71446 337-239-3401 FAX 337-239-7507 APPLICATION FOR SUPPORT PERSONNEL **************************************************************** PLEASE
VERNON PARISH SCHOOL SYSTEM 201 BELVIEW ROAD LEESVILLE, LA 71446 337-239-3401 FAX 337-239-7507 APPLICATION FOR SUPPORT PERSONNEL **************************************************************** PLEASE
Instructions for Employment Eligibility Verification
 Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
LETTER OF REASONABLE ASSURANCE
 LETTER OF REASONABLE ASSURANCE To: From: Substitute Teachers/Substitute Paraprofessionals James D. Baker, Director of Human Resources This letter provides notice of reasonable assurance of continued employment
LETTER OF REASONABLE ASSURANCE To: From: Substitute Teachers/Substitute Paraprofessionals James D. Baker, Director of Human Resources This letter provides notice of reasonable assurance of continued employment
Employment Application
 Employment Application CorrBox INCORPORATED 24551 Del Prado #639 Dana Point, CA 92629 Tel. (949) 248-5880 Fax. (949) 373-3256 info@corrbox.com Applicant Information Last First M.I. Date: Street Address
Employment Application CorrBox INCORPORATED 24551 Del Prado #639 Dana Point, CA 92629 Tel. (949) 248-5880 Fax. (949) 373-3256 info@corrbox.com Applicant Information Last First M.I. Date: Street Address
Instructions Read all instructions carefully before completing this form.
 Department of Homeland Security U.S. Citizenship and Immigration Services OMB No. 1615-0047;; Expires 08/31/12 Form I-9, Employment Eligibility Verification Instructions Read all instructions carefully
Department of Homeland Security U.S. Citizenship and Immigration Services OMB No. 1615-0047;; Expires 08/31/12 Form I-9, Employment Eligibility Verification Instructions Read all instructions carefully
Are you a current WVU student? (Circle One)
") \X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: Legal First
\X,est'vlrginialJnivetSil}' Employee Information Form Benefits Eligible: o NO o YES Session:_/_/_@_ AM PM Personal Information (Please Print) Gender: (check one) omale o Female Today's Date: Legal First
Payroll New Hire and Status Change Form
 Payroll New Hire and Status Change Form Employer name: Employer location (if applicable): Action (mark one): Add Terminate Change Transfer Employee name: Address: (Write See W-4 Form if you are attaching)
Payroll New Hire and Status Change Form Employer name: Employer location (if applicable): Action (mark one): Add Terminate Change Transfer Employee name: Address: (Write See W-4 Form if you are attaching)
SUBSTITUTE TEACHER APPLICATION
 501 Pacific Avenue Bremen, GA 30110 770-537-5508 SUBSTITUTE TEACHER APPLICATION LAST NAME FIRST MIDDLE DATE STREET ADDRESS CITY STATE ZIP TELEPHONE NUMBER EMAIL ADDRESS CURRENT EMPLOYER: HIGHEST EDUCATION
501 Pacific Avenue Bremen, GA 30110 770-537-5508 SUBSTITUTE TEACHER APPLICATION LAST NAME FIRST MIDDLE DATE STREET ADDRESS CITY STATE ZIP TELEPHONE NUMBER EMAIL ADDRESS CURRENT EMPLOYER: HIGHEST EDUCATION
I-9 Process GuIde Alka Bahal, Esq.
 Alka Bahal, Esq. Partner & Co-Chair, Corporate Immigration Practice Direct: 973.994.7800 Fax: 973.992.1653 immigration@foxrothschild.com Table of Contents Introduction...3 Procedures...4 Section 1: Employee...4
Alka Bahal, Esq. Partner & Co-Chair, Corporate Immigration Practice Direct: 973.994.7800 Fax: 973.992.1653 immigration@foxrothschild.com Table of Contents Introduction...3 Procedures...4 Section 1: Employee...4
Instructions for Employment Eligibility Verification
 Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form 1-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form 1-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
I-9 REFERENCE GUIDE. Student Employment For the employing department: Completing Section 2 January, 2017
 I-9 REFERENCE GUIDE Student Employment For the employing department: Completing Section 2 January, 2017 THE FORM I-9 According to Federal Law, all persons working for a new employer are required to show
I-9 REFERENCE GUIDE Student Employment For the employing department: Completing Section 2 January, 2017 THE FORM I-9 According to Federal Law, all persons working for a new employer are required to show
Employment Eligibility Verification
 Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 START HERE: Read instructions carefully
I-9 Reference Guide. Student Employment For the student employee: Completing Section 1 January, 2017
 I-9 Reference Guide Student Employment For the student employee: Completing Section 1 January, 2017 The Form I-9 According to Federal Law, all persons working for a new employer are required to show original
I-9 Reference Guide Student Employment For the student employee: Completing Section 1 January, 2017 The Form I-9 According to Federal Law, all persons working for a new employer are required to show original
I-9 REFERENCE GUIDE. Student Employment For the employing department: Completing Section 2 December, 2015
 I-9 REFERENCE GUIDE Student Employment For the employing department: Completing Section 2 December, 2015 THE FORM I-9 According to Federal Law, all persons working for a new employer are required to show
I-9 REFERENCE GUIDE Student Employment For the employing department: Completing Section 2 December, 2015 THE FORM I-9 According to Federal Law, all persons working for a new employer are required to show
GEORGIA DEPARTMENT OF CORRECTIONS Standard Operating Procedures
 Policy Number: 104.13 Effective Date: 8/28/2018 Page Number: 1 of 6 I. Introduction and Summary: Employees, hired or re-hired by the Georgia Department of Corrections (GDC), must be authorized to work
Policy Number: 104.13 Effective Date: 8/28/2018 Page Number: 1 of 6 I. Introduction and Summary: Employees, hired or re-hired by the Georgia Department of Corrections (GDC), must be authorized to work
Employment Eligibility Verification (Form I-9)
") crosscountry.com Employment Eligibility Verification (Form I-9) To ensure that Employment Eligibility Verification Form I-9 is completed in accordance with the Department of Homeland Security - U.S. Citizenship
crosscountry.com Employment Eligibility Verification (Form I-9) To ensure that Employment Eligibility Verification Form I-9 is completed in accordance with the Department of Homeland Security - U.S. Citizenship
Employment Application
 Employment Application IMPORTANT Instructions for completing the application form. 1. Type or print clearly in black or blue ink. 2. Answer every question fully and accurately. If not applicable, please
Employment Application IMPORTANT Instructions for completing the application form. 1. Type or print clearly in black or blue ink. 2. Answer every question fully and accurately. If not applicable, please
Complete Form I-9 Section 2:
 This job aid will assist you in completing Section 2 of the Form I-9 in Workday. The form has a government mandated due date of 3 days after the hire date. All documents presented to you by the new hire
This job aid will assist you in completing Section 2 of the Form I-9 in Workday. The form has a government mandated due date of 3 days after the hire date. All documents presented to you by the new hire
The non-photo ID options in List B do not apply to minors pursuing employment with E-Verify companies.
 The Department of Homeland Security has issued an updated form I-9 that went into effect on January 22, 2017. This version requires minors (individuals 17 or under) to meet the same requirements as adults
The Department of Homeland Security has issued an updated form I-9 that went into effect on January 22, 2017. This version requires minors (individuals 17 or under) to meet the same requirements as adults
Please provide the full legal name of the employee (as it appears on your income tax return or social security card)
") EMPLOYEE WORKSHEET EMPLOYEE CONTACT INFORMATION: Name of Employer: Please provide the full legal name of the employee (as it appears on your income tax return or social security card) Mr. First Name M.I.
EMPLOYEE WORKSHEET EMPLOYEE CONTACT INFORMATION: Name of Employer: Please provide the full legal name of the employee (as it appears on your income tax return or social security card) Mr. First Name M.I.
REDMOND MUNICIPAL AIRPORT INITIAL ID APPLICATION AOA ID
 REDMOND MUNICIPAL AIRPORT INITIAL ID APPLICATION AOA ID AIRPORT USE - DATE RECEIVED NAME: LAST NAME LEGAL FIRST NAME MIDDLE NAME ALL - NICK NAMES / FORMER NAMES / ALIAS: ID PIN = LAST - 4 OF SSN OR PHONE
REDMOND MUNICIPAL AIRPORT INITIAL ID APPLICATION AOA ID AIRPORT USE - DATE RECEIVED NAME: LAST NAME LEGAL FIRST NAME MIDDLE NAME ALL - NICK NAMES / FORMER NAMES / ALIAS: ID PIN = LAST - 4 OF SSN OR PHONE
Immigration Reform and Control Act (IRCA)
") REVISED 04/05/2016 PAGE 1 OF 5 Immigration Reform and Control Act (IRCA) Compliance To comply with IRCA federal regulations, all employees are required to complete an Employment Eligibility Verification
REVISED 04/05/2016 PAGE 1 OF 5 Immigration Reform and Control Act (IRCA) Compliance To comply with IRCA federal regulations, all employees are required to complete an Employment Eligibility Verification
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT 14102 Pine Meadow LN Tomball, TX 77377 Mailing: PO Box 1988 Tomball, TX 77377 1988 Tel: 281 290 8335 Fax: 281 290 8336 Email: info@challengerdrilling.com (PLEASE PRINT CLEARLY
APPLICATION FOR EMPLOYMENT 14102 Pine Meadow LN Tomball, TX 77377 Mailing: PO Box 1988 Tomball, TX 77377 1988 Tel: 281 290 8335 Fax: 281 290 8336 Email: info@challengerdrilling.com (PLEASE PRINT CLEARLY
Employment Application
 Employment Application APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State ZIP E-mail Date Available Social Security No. Desired Salary Position Applied for Are you a citizen
Employment Application APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State ZIP E-mail Date Available Social Security No. Desired Salary Position Applied for Are you a citizen
CITY OF SHERIDAN, WYOMING
 CITY OF SHERIDAN, WYOMING Office Use Only Received: HUMAN RESOURCES DEPARTMENT Phone: (307) 674-6483 (Please Use for mailing) Fax: (307) 675-4270 55 Grinnell Plaza, P.O. Box 848 Email: hdoke@sheridanwy.net
CITY OF SHERIDAN, WYOMING Office Use Only Received: HUMAN RESOURCES DEPARTMENT Phone: (307) 674-6483 (Please Use for mailing) Fax: (307) 675-4270 55 Grinnell Plaza, P.O. Box 848 Email: hdoke@sheridanwy.net
APPENDIX A. I-9 Requirements Document List
 APPENDIX A I-9 Requirements Document List Ever since the passage of the Immigration Reform and Control Act in 1986, employers have had to verify the employment authorization of each employee they hire.
APPENDIX A I-9 Requirements Document List Ever since the passage of the Immigration Reform and Control Act in 1986, employers have had to verify the employment authorization of each employee they hire.
Pre-employment: Drug test, immunizations, and TB will be verified. Your background will be ran. (For GRIC members, a GRIC background will be ran as
 Pre-employment: Drug test, immunizations, and TB will be verified. Your background will be ran. (For GRIC members, a GRIC background will be ran as well.) 7-10 Business Days TB, drug test, and background(s)
Pre-employment: Drug test, immunizations, and TB will be verified. Your background will be ran. (For GRIC members, a GRIC background will be ran as well.) 7-10 Business Days TB, drug test, and background(s)
Instructions for Form I-9, Employment Eligibility Verification
 Instructions for Form I-9, Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 Anti-Discrimination
Instructions for Form I-9, Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 08/31/2019 Anti-Discrimination
CITY OF SHERIDAN, WYOMING
 CITY OF SHERIDAN, WYOMING Office Use Only Received: HUMAN RESOURCES DEPARTMENT Phone: (307) 674-6483 (Please Use for mailing) Fax: (307) 675-4270 55 East Grinnell, P.O. Box 848 Email: hdoke@sheridanwy.net
CITY OF SHERIDAN, WYOMING Office Use Only Received: HUMAN RESOURCES DEPARTMENT Phone: (307) 674-6483 (Please Use for mailing) Fax: (307) 675-4270 55 East Grinnell, P.O. Box 848 Email: hdoke@sheridanwy.net
NON SIDA VEHICLE ACCESS BADGE/GA
 P INSTRUCTIONS FOR FILLING OUT THE BOISE AIR TERMINAL - APPLICATION FOR NON SIDA VEHICLE ACCESS BADGE/GA Revised October 19, 2016 P NOTE: The application must be filled out legibly and completely. If not,
P INSTRUCTIONS FOR FILLING OUT THE BOISE AIR TERMINAL - APPLICATION FOR NON SIDA VEHICLE ACCESS BADGE/GA Revised October 19, 2016 P NOTE: The application must be filled out legibly and completely. If not,
Camp Dudley at Kiniya - Voluntary Disclosure Statement This disclosure statement must be updated yearly.
 Camp Dudley at Kiniya - Voluntary Disclosure Statement This disclosure statement must be updated yearly. Name Birth date Last First Middle Home address Street Address City State Zip Social Security # Other
Camp Dudley at Kiniya - Voluntary Disclosure Statement This disclosure statement must be updated yearly. Name Birth date Last First Middle Home address Street Address City State Zip Social Security # Other
GENERAL AVIATION APPLICATION
 GENERAL AVIATION APPLICATION INSTRUCTION SHEET FOR COMPLETING THE BOISE AIRPORT GA APPLICATION (Revised October 2017) The application must be filled out legibly and completely. If not, the application
GENERAL AVIATION APPLICATION INSTRUCTION SHEET FOR COMPLETING THE BOISE AIRPORT GA APPLICATION (Revised October 2017) The application must be filled out legibly and completely. If not, the application
Instructions for Employment Eligibility Verification
 Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
Instructions for Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form I-9 OMB No. 1615-0047 Expires 03/31/2016 Read all instructions
AIRPORT SECURITY IDENTIFICATION BADGE APPLICATION
 AIRPORT SECURITY IDENTIFICATION BADGE APPLICATION PRINT all information in the box below before returning this form to the Airport Operations Control Center. NAME (LAST, FIRST, MIDDLE) G ALIAS(ES) SOCIAL
AIRPORT SECURITY IDENTIFICATION BADGE APPLICATION PRINT all information in the box below before returning this form to the Airport Operations Control Center. NAME (LAST, FIRST, MIDDLE) G ALIAS(ES) SOCIAL
To schedule an Application Processing Appointment
 REDMOND MUNICIPAL AIRPORT (RDM) Secured & Sterile Area ID Application THIS PAGE FOR APPLICANT TO KEEP Identification badges issued by Redmond Municipal Airport (RDM) are, and remain, property of the Airport.
REDMOND MUNICIPAL AIRPORT (RDM) Secured & Sterile Area ID Application THIS PAGE FOR APPLICANT TO KEEP Identification badges issued by Redmond Municipal Airport (RDM) are, and remain, property of the Airport.
INSTRUCTIONS FOR FILLING OUT THE BOISE AIR TERMINAL - APPLICATION FOR NON SIDA AOA ACCESS BADGE. Revised October 19, 2016
 AOA INSTRUCTIONS FOR FILLING OUT THE BOISE AIR TERMINAL - APPLICATION FOR NON SIDA AOA ACCESS BADGE Revised October 19, 2016 AOA NOTE: The application must be filled out legibly and completely. If not,
AOA INSTRUCTIONS FOR FILLING OUT THE BOISE AIR TERMINAL - APPLICATION FOR NON SIDA AOA ACCESS BADGE Revised October 19, 2016 AOA NOTE: The application must be filled out legibly and completely. If not,
GENERAL AVIATION ACCESS APPLICATION
 GENERAL AVIATION ACCESS APPLICATION Updated November 2018 DRIVERS LICENSE COMPANY: No L NM M FOR OFFICIAL USE ONLY Accounting Form Received & Reviewed Received/ Reviewed Application Appropriate Forms of
GENERAL AVIATION ACCESS APPLICATION Updated November 2018 DRIVERS LICENSE COMPANY: No L NM M FOR OFFICIAL USE ONLY Accounting Form Received & Reviewed Received/ Reviewed Application Appropriate Forms of
USCIS permits forms to be printed on both sides (as is the actual printed form provided by USCIS) or on single sides.
 or on single sides.") Chapter 2 - Completing the the I-9 I-9 Form 2.1 Where can I I obtain a a Form I-9? I-9? USCIS makes the Form I-9 available for download on its website in a PDF format at www.uscis.gov. The form can also
Chapter 2 - Completing the the I-9 I-9 Form 2.1 Where can I I obtain a a Form I-9? I-9? USCIS makes the Form I-9 available for download on its website in a PDF format at www.uscis.gov. The form can also
Melbourne International Airport Police Department Security Badge Application SIDA SECURE Area
 Melbourne International Airport Police Department Security Badge Application SIDA SECURE Area Revision : June, 2009 Prior to issuance of an Airport Security Identification Media the U.S. Department of
Melbourne International Airport Police Department Security Badge Application SIDA SECURE Area Revision : June, 2009 Prior to issuance of an Airport Security Identification Media the U.S. Department of
NAVIGATE THE I-9 RULES LIKE A VIKING TO AVOID SINKING YOUR BUSINESS IN LAWSUITS AND PENALTIES
 NAVIGATE THE I-9 RULES LIKE A VIKING TO AVOID SINKING YOUR BUSINESS IN LAWSUITS AND PENALTIES Presented by: Roxana E. Verano, Esq. Rodrigo J. Torres, Esq. Landegger Baron Law Group, ALC Exclusively Representing
NAVIGATE THE I-9 RULES LIKE A VIKING TO AVOID SINKING YOUR BUSINESS IN LAWSUITS AND PENALTIES Presented by: Roxana E. Verano, Esq. Rodrigo J. Torres, Esq. Landegger Baron Law Group, ALC Exclusively Representing
FORM I-9: REFRESHER TRAINING. CWD October 2018
 FORM I-9: REFRESHER TRAINING CWD October 2018 Today s Agenda I. What s an I-9 II. Harvard s Process: New Hires, Re-Certification III. Verifying and Listing Documents in Section 2 IV. Review the I-9 Visa
FORM I-9: REFRESHER TRAINING CWD October 2018 Today s Agenda I. What s an I-9 II. Harvard s Process: New Hires, Re-Certification III. Verifying and Listing Documents in Section 2 IV. Review the I-9 Visa
Immigration Compliance
 Immigration Compliance Davis C. Bae Regional Managing Partner, Fisher Phillips dbae@ / (206) 693-5060 Robert Gibbs Partner, Gibbs Houston Pauw rgibbs@ghp-law.net/ (206)224-8790 ICE Growth and Directives
Immigration Compliance Davis C. Bae Regional Managing Partner, Fisher Phillips dbae@ / (206) 693-5060 Robert Gibbs Partner, Gibbs Houston Pauw rgibbs@ghp-law.net/ (206)224-8790 ICE Growth and Directives
Instructions for Form 1-9, Employment Eligibility Verification. Department of Homeland Security U.S. Citizenship and Immigration Services
 Instructions for Form 1-9, Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form 1-9 OMB No. 1615-0047 Expires 08/31/2019 Anti-Discrimination
Instructions for Form 1-9, Employment Eligibility Verification Department of Homeland Security U.S. Citizenship and Immigration Services USCIS Form 1-9 OMB No. 1615-0047 Expires 08/31/2019 Anti-Discrimination
USCIS Revises Employment Eligibility Verification Form I-9 Revision will eliminate certain documents for employment verification
 Office of Communications Fact Sheet November 7, 2007 (Revised) USCS Revises Employment Eligibility Verification Form -9 Revision will eliminate certain documents for employment verification U.S. Citizenship
Office of Communications Fact Sheet November 7, 2007 (Revised) USCS Revises Employment Eligibility Verification Form -9 Revision will eliminate certain documents for employment verification U.S. Citizenship
EMPLOYEE: NEW HIRE PACKET INSTRUCTIONS & CHECKLIST
 EMPLOYEE: NEW HIRE PACKET INSTRUCTIONS & CHECKLIST These forms are electronically-fillable but must be printed and signed. They may be completed by hand if preferred. For the I-9 Employment Eligibility
EMPLOYEE: NEW HIRE PACKET INSTRUCTIONS & CHECKLIST These forms are electronically-fillable but must be printed and signed. They may be completed by hand if preferred. For the I-9 Employment Eligibility
I-9 and Work Authorization
 I-9 and Work Authorization September 14, 2017 Office of General Counsel Daniel McCabe Assistant General Counsel Section 1: I-9 s Generally 2 Form I-9 Generally Since 1986, employees in the U.S. have filled
I-9 and Work Authorization September 14, 2017 Office of General Counsel Daniel McCabe Assistant General Counsel Section 1: I-9 s Generally 2 Form I-9 Generally Since 1986, employees in the U.S. have filled
Part Seven Some Questions You May Have About Form I-9
 Part Seven Some Questions You May Have About Form I-9 Employers should read these questions and answers carefully. They contain valuable information that, in some cases, is not found elsewhere in this
Part Seven Some Questions You May Have About Form I-9 Employers should read these questions and answers carefully. They contain valuable information that, in some cases, is not found elsewhere in this
MSU Child Development Laboratories Hiring Packet
 MSU Child Development Laboratories Hiring Packet College of Social Science Department of Human Development and Family Studies Child Development Laboratories East Lansing Campus Central School 325 W. Grand
MSU Child Development Laboratories Hiring Packet College of Social Science Department of Human Development and Family Studies Child Development Laboratories East Lansing Campus Central School 325 W. Grand
EMPLOYMENT VERIFICATION, INVESTIGATIONS, AND AUDITS
 EMPLOYMENT VERIFICATION, INVESTIGATIONS, AND AUDITS Presented by: Derek Illar Associate Eckert Seamans Cherin & Mellott, LLC 600 Grant Street, 44 th Floor Pittsburgh, PA 15219 (412) 566 6771 dillar@eckertseamans.com
EMPLOYMENT VERIFICATION, INVESTIGATIONS, AND AUDITS Presented by: Derek Illar Associate Eckert Seamans Cherin & Mellott, LLC 600 Grant Street, 44 th Floor Pittsburgh, PA 15219 (412) 566 6771 dillar@eckertseamans.com
This packet includes the following documents:
 This packet includes the following documents: - Instruction Sheet/Checklist Letter of Instruction Security Badge Application Form Authorized Issuer and GBRAA Use Only Page - SIDA and Sterile Area Worker
This packet includes the following documents: - Instruction Sheet/Checklist Letter of Instruction Security Badge Application Form Authorized Issuer and GBRAA Use Only Page - SIDA and Sterile Area Worker
WIA Youth Eligibility Reference List
 Applicant Name: Application Date: Completed By: Reviewed By: See VWL 13-03 for information on limited acceptance of self-certification ( self-attestation ) for Youth applicants in Extreme Circumstances.
Applicant Name: Application Date: Completed By: Reviewed By: See VWL 13-03 for information on limited acceptance of self-certification ( self-attestation ) for Youth applicants in Extreme Circumstances.
Commonwealth of Massachusetts
 Commonwealth of Massachusetts STATE EMPLOYMENT APPLICATION FOR: www.mass.gov/massdot SEASONAL TOLL COLLECTOR - 2012 All applicants are required to submit the following: Completed MassDOT Employment Application;
Commonwealth of Massachusetts STATE EMPLOYMENT APPLICATION FOR: www.mass.gov/massdot SEASONAL TOLL COLLECTOR - 2012 All applicants are required to submit the following: Completed MassDOT Employment Application;
BOISE AIR TERMINAL APPLICATION FOR SAAB ACCESS
 BOISE AIR TERMINAL APPLICATION FOR SAAB ACCESS Revised November 2018 TYPE- Smart Card Employer: For Office Use Only DATE INIT DATE INIT Accounting Form Received & Reviewed Fingerprint Received Received/
BOISE AIR TERMINAL APPLICATION FOR SAAB ACCESS Revised November 2018 TYPE- Smart Card Employer: For Office Use Only DATE INIT DATE INIT Accounting Form Received & Reviewed Fingerprint Received Received/
Attachment J WIOA Eligibility Checklist for In-School Youth
 The Virginia Community College System VIRGINIA WORKFORCE LETTER (VWL) #15-02 Title: Eligibility Guidelines Attachment J WIOA Eligibility Checklist for In-School Youth Applicant Name: Application Date:
The Virginia Community College System VIRGINIA WORKFORCE LETTER (VWL) #15-02 Title: Eligibility Guidelines Attachment J WIOA Eligibility Checklist for In-School Youth Applicant Name: Application Date:
To obtain an Occupational Tax Certificate, follow the instructions below. 1. The Occupational Tax Application form and New Business form.
 To obtain an Occupational Tax Certificate, follow the instructions below. Return the Following Completed Documents 1. The Occupational Tax Application form and New Business form. 2. The Emergency Information
To obtain an Occupational Tax Certificate, follow the instructions below. Return the Following Completed Documents 1. The Occupational Tax Application form and New Business form. 2. The Emergency Information
Information Memorandum Transmittal
 Children, Adults and Families Information Memorandum Transmittal Karen House, Program Manager SS Medical Programs Number: SS-IM-07-001 Authorized Signature Issue Date: 01/04/2007 Topic: Medical Benefits
Children, Adults and Families Information Memorandum Transmittal Karen House, Program Manager SS Medical Programs Number: SS-IM-07-001 Authorized Signature Issue Date: 01/04/2007 Topic: Medical Benefits
Contact: CMS Public Affairs July 06, 2006 (202) HHS ISSUES FINAL REGULATIONS WITH COMMENT ON CITIZENSHIP GUIDELINES FOR MEDICAID ELIGIBIITY
 HHS ISSUES FINAL REGULATIONS WITH COMMENT ON CITIZENSHIP GUIDELINES FOR MEDICAID ELIGIBIITY") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Public Affairs Office MEDICAID FACT SHEET Contact: CMS Public
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Public Affairs Office MEDICAID FACT SHEET Contact: CMS Public
WIA Eligibility Checklist for Adults and Dislocated Workers
 Applicant Name: Application Date: Completed by: Reviewed by: See VWL 13 03 for information on limited acceptance of self certification ( self attestation ) for Adult and Dislocated Worker applicants in
Applicant Name: Application Date: Completed by: Reviewed by: See VWL 13 03 for information on limited acceptance of self certification ( self attestation ) for Adult and Dislocated Worker applicants in
L.G. Hanscom Field SIDA Identification Badge Process
 L.G. Hanscom Field SIDA Identification Badge Process The ID badge process entails several steps: the application completion and submission, a fingerprint scan with a Security Threat Assessment (STA) and
L.G. Hanscom Field SIDA Identification Badge Process The ID badge process entails several steps: the application completion and submission, a fingerprint scan with a Security Threat Assessment (STA) and
Please provide the full legal name of the employee (as it appears on your income tax return or social security card)
") EMPLOYEE WORKSHEET EMPLOYEE CONTACT INFORMATION: Name of Employer: Please provide the full legal name of the employee (as it appears on your income tax return or social security card) Mr. First Name M.I.
EMPLOYEE WORKSHEET EMPLOYEE CONTACT INFORMATION: Name of Employer: Please provide the full legal name of the employee (as it appears on your income tax return or social security card) Mr. First Name M.I.
GEORGIA BOARD OF PHARMACY A Division of the Georgia Department of Community Health 2 Peachtree Street, N.W. 6 th Floor Atlanta, Georgia 30303
 GEORGIA BOARD OF PHARMACY A Division of the Georgia Department of Community Health 2 Peachtree Street, N.W. 6 th Floor Atlanta, Georgia 30303 PHARMACIST APPLICANT INFORMATION SHEET dates are available
GEORGIA BOARD OF PHARMACY A Division of the Georgia Department of Community Health 2 Peachtree Street, N.W. 6 th Floor Atlanta, Georgia 30303 PHARMACIST APPLICANT INFORMATION SHEET dates are available
South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Long Term Health Care Administrators
 South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Long Term Health Care Administrators 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone:
South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Long Term Health Care Administrators 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone:
Northwest Workforce Council
 Northwest Workforce Council POLICY AND PROCEDURE DIRECTIVE EFFECTIVE DATE: July 1, 2015 SUBJECT: Eligibility Verification and Priority Selection for Title I-B Young Adults (Youth) REFERENCE #: WIOA 01-15
Northwest Workforce Council POLICY AND PROCEDURE DIRECTIVE EFFECTIVE DATE: July 1, 2015 SUBJECT: Eligibility Verification and Priority Selection for Title I-B Young Adults (Youth) REFERENCE #: WIOA 01-15
CPA LICENSURE APPLICATION BY RECIPROCITY ELECTRONIC APPLICATION FORMS AND INSTRUCTIONS
 South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Accountancy 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone: 803-896-4770 Contact.Accountancy@llr.sc.gov
South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Accountancy 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone: 803-896-4770 Contact.Accountancy@llr.sc.gov
Inividuals may be prosecuted for knowingly and willfully entering false information on. the form. Employers are responsible for

Welcome to Prince William County Public Schools!
 . Welcome to Prince William County Public Schools! The information in this hiring packet is intended for applicants who are under the age of 18. As a condition of employment, you must attend a mandatory
. Welcome to Prince William County Public Schools! The information in this hiring packet is intended for applicants who are under the age of 18. As a condition of employment, you must attend a mandatory
Are There Cases When You Should Not Use This Form? What Information Is Needed to Search for USCIS Records? Verification of Identity in Person.
 Department of Homeland Security U.S. Citizenship and Immigration Services OMB No. 1653-0030; Expires 08/31/05 G-639, Freedom of Information/ Privacy Act Request Instructions NOTE: Please read all Instructions
Department of Homeland Security U.S. Citizenship and Immigration Services OMB No. 1653-0030; Expires 08/31/05 G-639, Freedom of Information/ Privacy Act Request Instructions NOTE: Please read all Instructions
... moves to amend H.F. No. 3959, the third engrossment, as follows:
 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8... moves to amend H.F. No. 3959, the third engrossment, as follows: Delete everything after the enacting clause and insert: "Section 1. Minnesota Statutes 2014, section
1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8... moves to amend H.F. No. 3959, the third engrossment, as follows: Delete everything after the enacting clause and insert: "Section 1. Minnesota Statutes 2014, section
Attachment I WIOA Eligibility Checklist for Adults and Dislocated Workers
 The Virginia Community College System VIRGINIA WORKFORCE LETTER (VWL) #15-02 Title: Eligibility Guidelines Attachment I WIOA Eligibility Checklist for Adults and Dislocated Workers Applicant Name: Application
The Virginia Community College System VIRGINIA WORKFORCE LETTER (VWL) #15-02 Title: Eligibility Guidelines Attachment I WIOA Eligibility Checklist for Adults and Dislocated Workers Applicant Name: Application
AIRPORT IDENTIFICATION BADGE APPLICATION
 Airport Badge Types INSTRUCTIONS AOA Badge All individuals who require regular and routine access to the Airport Operations Area (AOA), which includes all areas of the airport inside the perimeter fencing
Airport Badge Types INSTRUCTIONS AOA Badge All individuals who require regular and routine access to the Airport Operations Area (AOA), which includes all areas of the airport inside the perimeter fencing
EMPLOYMENT/CONTRACTOR APPLICATION
 For Official Use Only Date Received:, 2013 Reviewed by: Comments: INTERVIEWED BY: TRAINING RIDEALONG: SUBMITTED MVR TO INSURANCE: DATE: MVR QUALIFY?: EMPLOYMENT/CONTRACTOR APPLICATION Payback Repo Inc.
For Official Use Only Date Received:, 2013 Reviewed by: Comments: INTERVIEWED BY: TRAINING RIDEALONG: SUBMITTED MVR TO INSURANCE: DATE: MVR QUALIFY?: EMPLOYMENT/CONTRACTOR APPLICATION Payback Repo Inc.
STUDENT PERMIT APPLICATION INSTRUCTIONS
 South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Barber Examiners 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone: 803-896-4588 BoardInfo@llr.sc.gov
South Carolina Department of Labor, Licensing and Regulation South Carolina Board of Barber Examiners 110 Centerview Dr. Columbia SC 29210 P.O. Box 11329 Columbia SC 29211-1329 Phone: 803-896-4588 BoardInfo@llr.sc.gov
FILLING OUT THE APPLICATION PAGE 1
 INSTRUCTION SHEET FOR FILLING OUT THE BOISE AIRPORT SIDA APPLICATION (Revised March 16, 2016) NOTE: The application must be filled out legibly and completely. If not, the application will not be processed
INSTRUCTION SHEET FOR FILLING OUT THE BOISE AIRPORT SIDA APPLICATION (Revised March 16, 2016) NOTE: The application must be filled out legibly and completely. If not, the application will not be processed
Access to Health Coverage for Immigrants Living with HIV Quick Reference Guide
 Access to Health Coverage for Immigrants Living with HIV Quick Reference Guide Are you working with immigrants living with HIV who need health coverage? Use this quick reference guide to learn about these
Access to Health Coverage for Immigrants Living with HIV Quick Reference Guide Are you working with immigrants living with HIV who need health coverage? Use this quick reference guide to learn about these
Broadcast to All DPA Staff, DPA State Associates, and OCS Eligibility Staff From Policy and Program Development
 Broadcast to All DPA Staff, DPA State Associates, and OCS Eligibility Staff From Policy and Program Development This broadcast provides initial instructions for implementing the new citizenship and identity
Broadcast to All DPA Staff, DPA State Associates, and OCS Eligibility Staff From Policy and Program Development This broadcast provides initial instructions for implementing the new citizenship and identity
To qualify for a Chicago CityKey, you must be a resident of Chicago and meet the following document criteria:
 APPLICANT DOCUMENT GUIDE CityKey Use this document guide when you are completing the: Application for the City of Chicago Municipal ID Program-CityKey To qualify for a Chicago CityKey, you must be a resident
APPLICANT DOCUMENT GUIDE CityKey Use this document guide when you are completing the: Application for the City of Chicago Municipal ID Program-CityKey To qualify for a Chicago CityKey, you must be a resident
Workforce Innovation and Opportunity Act Title IB Eligibility Policies will be in effect starting July 1, Eligibility policies are considered
 Workforce Innovation and Opportunity Act Title IB Eligibility Policies will be in effect starting July 1, 2015. Eligibility policies are considered working drafts until the Northwest Workforce Council
Workforce Innovation and Opportunity Act Title IB Eligibility Policies will be in effect starting July 1, 2015. Eligibility policies are considered working drafts until the Northwest Workforce Council
WV INCOME MAINTENANCE MANUAL. Verification
 CITIZENSHIP AND IDENTITY REQUIREMENTS Section 6036 of the Deficit Reduction Act of 2005 (DRA) enacted on February 8, 2006, requires individuals who claim United States citizenship to provide documentary
CITIZENSHIP AND IDENTITY REQUIREMENTS Section 6036 of the Deficit Reduction Act of 2005 (DRA) enacted on February 8, 2006, requires individuals who claim United States citizenship to provide documentary
Occupational License Application
 West Virginia Lottery Commission 900 Pennsylvania Avenue, Charleston, WV 25302 Occupational License Application INSTRUCTIONS This form is authorized under Article 22C of the 2007 West Virginia Lottery
West Virginia Lottery Commission 900 Pennsylvania Avenue, Charleston, WV 25302 Occupational License Application INSTRUCTIONS This form is authorized under Article 22C of the 2007 West Virginia Lottery
SECOND REGULAR SESSION [P E R F E C T E D] SENATE BILL NO TH GENERAL ASSEMBLY INTRODUCED BY SENATOR MUNZLINGER.
![SECOND REGULAR SESSION [P E R F E C T E D] SENATE BILL NO TH GENERAL ASSEMBLY INTRODUCED BY SENATOR MUNZLINGER.](/thumbs/94/118499469.jpg "SECOND REGULAR SESSION [P E R F E C T E D] SENATE BILL NO TH GENERAL ASSEMBLY INTRODUCED BY SENATOR MUNZLINGER.") SECOND REGULAR SESSION [P E R F E C T E D] SENATE BILL NO. 656 98TH GENERAL ASSEMBLY INTRODUCED BY SENATOR MUNZLINGER. Pre-filed December 1, 2015, and ordered printed. Read 2nd time January 7, 2016, and
SECOND REGULAR SESSION [P E R F E C T E D] SENATE BILL NO. 656 98TH GENERAL ASSEMBLY INTRODUCED BY SENATOR MUNZLINGER. Pre-filed December 1, 2015, and ordered printed. Read 2nd time January 7, 2016, and
Massachusetts Executive Office of Public Safety and Security. Statewide Applicant Fingerprint Identification Services (SAFIS) Program
 Program") Massachusetts Executive Office of Public Safety and Security Statewide Applicant Fingerprint Identification Services (SAFIS) Program Registration Guide Massachusetts Department of Children and Families
Massachusetts Executive Office of Public Safety and Security Statewide Applicant Fingerprint Identification Services (SAFIS) Program Registration Guide Massachusetts Department of Children and Families
CHAPTER 35. MEDICAL ASSISTANCE FOR
 CHAPTER 35. MEDICAL ASSISTANCE FOR ADULTS AND CHILDREN-ELIGIBILITY SUBCHAPTER 5. ELIGIBILITY AND COUNTABLE INCOME PART 3. NON-MEDICAL ELIGIBILITY REQUIREMENTS 317:35-5-25. Citizenship/alien status and
CHAPTER 35. MEDICAL ASSISTANCE FOR ADULTS AND CHILDREN-ELIGIBILITY SUBCHAPTER 5. ELIGIBILITY AND COUNTABLE INCOME PART 3. NON-MEDICAL ELIGIBILITY REQUIREMENTS 317:35-5-25. Citizenship/alien status and
SIDA APPLICATION. INSTRUCTION SHEET FOR COMPLETING THE BOISE AIRPORT SIDA APPLICATION (Revised October 2017)
") SIDA APPLICATION INSTRUCTION SHEET FOR COMPLETING THE BOISE AIRPORT SIDA APPLICATION (Revised October 2017) The application must be filled out legibly and completely. If not, the application will not be
SIDA APPLICATION INSTRUCTION SHEET FOR COMPLETING THE BOISE AIRPORT SIDA APPLICATION (Revised October 2017) The application must be filled out legibly and completely. If not, the application will not be
for fingerprint submitting agencies and contractors Prepared by the National Crime Prevention and Privacy Compact Council
 for fingerprint submitting agencies and contractors Prepared by the National Crime Prevention and Privacy Compact Council The National Crime Prevention and Privacy Compact Council (Compact Council) is
for fingerprint submitting agencies and contractors Prepared by the National Crime Prevention and Privacy Compact Council The National Crime Prevention and Privacy Compact Council (Compact Council) is
Attachment #1 - WIA ADULT ELIGIBILITY CRITERIA, GLOSSARY, AND DOCUMENTATION Revised October 2008
 Attachment #1 - WIA ADULT ELIGIBILITY CRITERIA, GLOSSARY, AND DOCUMENTATION Revised October 2008 Following is the eligibility criteria for the WIA Adult Program and a Glossary of relevant terms. Documentation
Attachment #1 - WIA ADULT ELIGIBILITY CRITERIA, GLOSSARY, AND DOCUMENTATION Revised October 2008 Following is the eligibility criteria for the WIA Adult Program and a Glossary of relevant terms. Documentation
First Division Engrossment
 HF1500 FIRST DIVISION This Document can be made available in alternative formats upon request 02/21/2019 State of Minnesota HOUSE OF REPRESENTATIVES First Division Engrossment 1500 NINETY-FIRST SESSION
HF1500 FIRST DIVISION This Document can be made available in alternative formats upon request 02/21/2019 State of Minnesota HOUSE OF REPRESENTATIVES First Division Engrossment 1500 NINETY-FIRST SESSION